Online & Home visit Consultation Available with Portable Home X-Ray facility available.
Consultation available on HINDI language also

🦴 Proximal Third Ulna Fracture in an Adolescent – A Clinical Overview
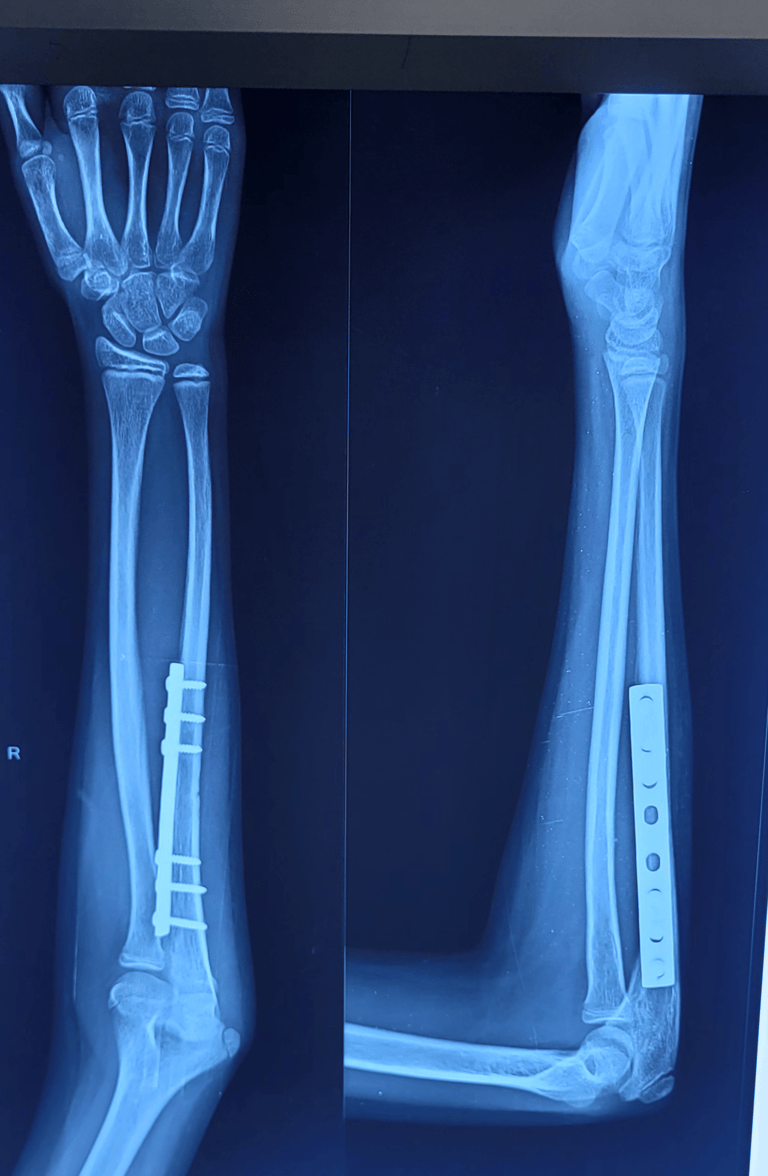
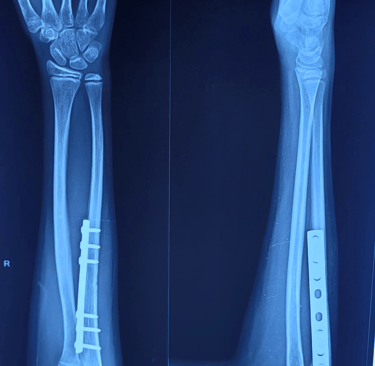
This X-ray demonstrates a fracture of the proximal third of the right ulna in an adolescent patient. The fracture is displaced with an unstable pattern, suggesting a moderate to high-energy injury.
Dr. M. Kalaivanan
5/26/20261 min read
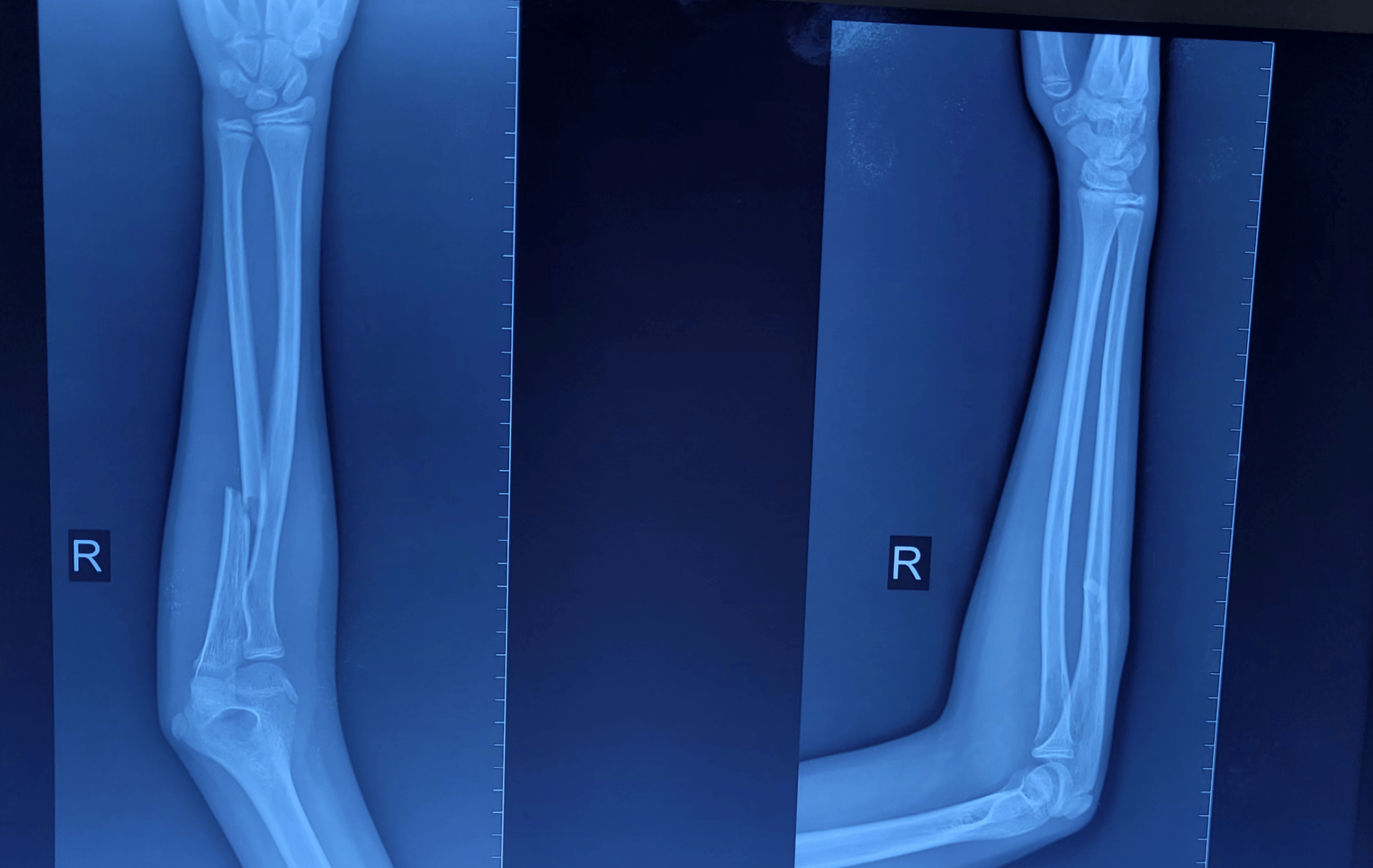
🦴 Proximal Third Ulna Fracture in an Adolescent – A Clinical Overview
📸 Case Summary
This X-ray demonstrates a fracture of the proximal third of the right ulna in an adolescent patient. The fracture is displaced with an unstable pattern, suggesting a moderate to high-energy injury.
(Proximal Ulna Fracture)
---
⚠️ Why This Injury Is Important
In children and adolescents, a proximal ulna fracture is rarely isolated. It is essential to always rule out an associated condition known as
👉 Monteggia fracture-dislocation
This involves:
• Fracture of the ulna
• Dislocation of the radial head at the elbow
❗ Important Note:
Missed diagnosis or inappropriate treatment (such as native oil bandaging without proper medical evaluation) can lead to long-term disability, deformity, and restricted elbow movement.
---
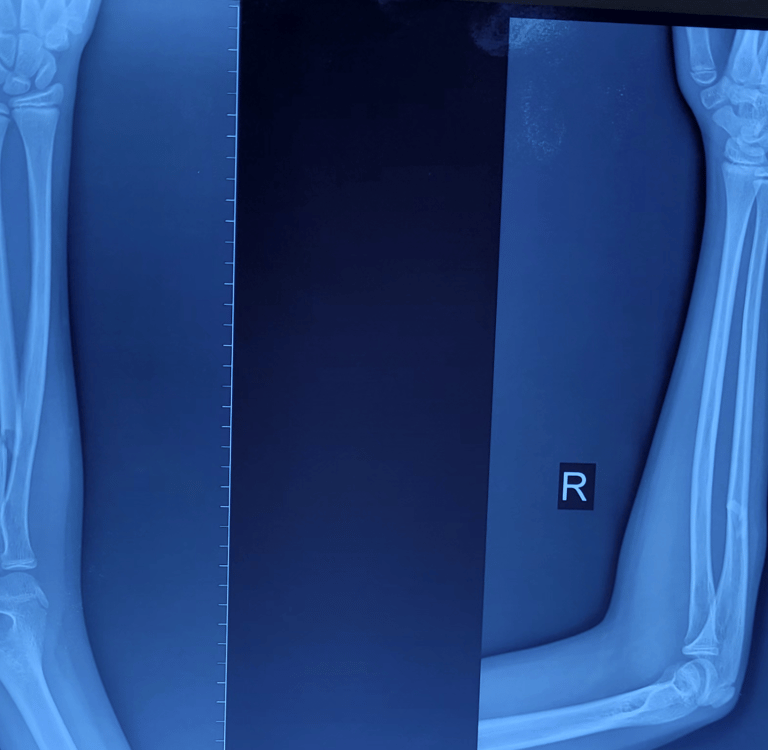
🔍 Understanding the Radiological Landmark
(Insert Annotated Elbow X-ray Image Here – Radiocapitellar Line)
This image highlights the key radiological lines used in evaluating elbow injuries:
📌 Important Lines to Remember
• Radiocapitellar Line
A line drawn along the axis of the radius
It should always pass through the capitellum
If it does not → suspect radial head dislocation
• Anterior Humeral Line
Drawn along the anterior cortex of the humerus
Should intersect the middle third of the capitellum
Useful in assessing supracondylar fractures
---
🔍 Key Radiological Assessment
👉 Orthopaedic specialist consultation is mandatory
• Evaluate fracture pattern (complete, displaced, comminuted)
• Check radiocapitellar alignment
• Assess for:
◦ Radial head dislocation
◦ Elbow joint congruity
◦ Associated neurovascular injury
---
🧠 Mechanism of Injury
• Fall on outstretched hand (FOOSH)
• Direct trauma to the forearm
• Sports-related injuries
---
🛠️ Management Approach
✅ If isolated, undisplaced ulna fracture:
• Conservative treatment with above-elbow slab/cast immobilization
• Regular follow-up with serial X-rays
⚠️ If displaced fracture or associated Monteggia injury:
• Urgent reduction is required
• Restoration of ulna length is the key principle
→ Radial head usually reduces automatically
• Surgical fixation (plate osteosynthesis) is recommended in unstable fractures for:
Early recovery
Better functional outcome
Early mobilization
---
⏳ Possible Complications
• Missed radial head dislocation
• Malunion of ulna
• Restricted forearm rotation
• Posterior interosseous nerve (PIN) injury
---
💡 Clinical Pearl
👉 “In pediatric forearm injuries, always fix the ulna first — the radius will follow.”
---
🏥 Expert Care Matters
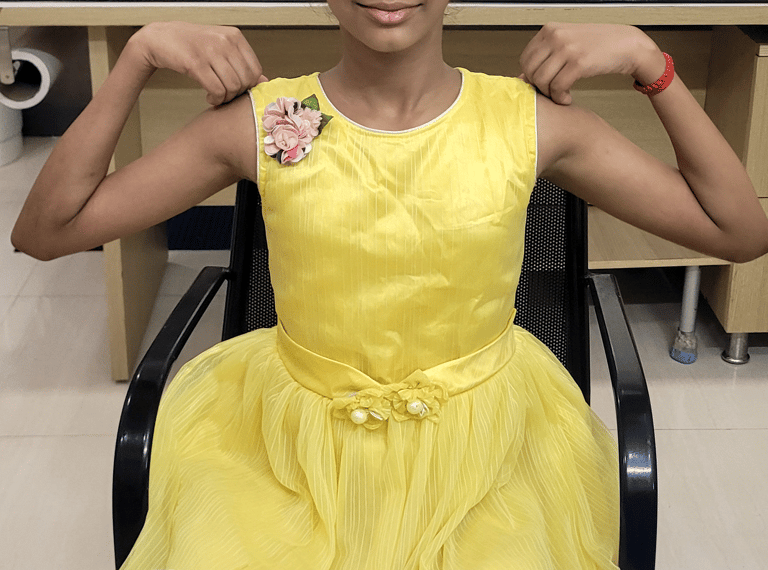
Early diagnosis and appropriate treatment ensure:
• Proper fracture healing
• Full restoration of elbow function
• Prevention of long-term deformity and disability
---
By
Dr. M. Kalaivanan, MS (Ortho)
Orthopaedic Surgeon – Trichy
📲 Call/WhatsApp: +91-8122073520
Get in touch
Sri Riddhi Specialty Clinic
Door no: 893, Kairasi Nagar, Rajiv Ghandhi Nagar Bustop, Vayalur Main Road, Natchikurichi, Tiruchirappalli - 620102
+91 99448 01540, +91 81220 73520
Consulting Hours
Monday- Saturday
05.30 PM-10.00 PM
On Sunday
Only on Appointment Basis